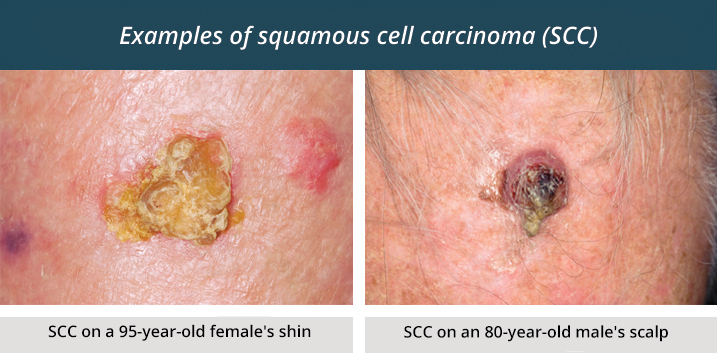
Squamous Cell Carcinoma (SCC) is the second most common form of skin cancer in Australia and is strongly linked to cumulative UV exposure. Unlike a Basal Cell Carcinoma (BCC), which typically grows slower and tends to remain localised - a SCC carries a real risk of deeper invasion and metastasis, particularly when it arises on high-risk sites such as the ear, lip, or scalp, or when the tumour is large, thick, or poorly differentiated.
SCCs often appear as:
Dr Schaefer regularly performs SCC removal procedures at Brisbane Private Hospital and in his rooms, both located in Spring Hill.
A biopsy confirms the diagnosis and provides essential information including tumour depth, degree of differentiation, presence of perineural invasion, and margin characteristics.
SCC excision is commonly performed under local anaesthesia for straightforward cases, while larger or complex lesions may require sedation or general anaesthesia.
The recommended margin depends on the risk category:
Margins for SCC are typically larger than those used for BCC, reflecting the higher potential for subclinical spread.
During surgery, the tumour and margin of healthy tissue are removed as a single specimen, carefully marked for orientation, and submitted for pathology. In select cases, particularly high-risk tumours in cosmetically sensitive locations, Mohs micrographic surgery may be recommended to achieve precise, real-time margin control while sparing as much healthy tissue as possible.
Once the SCC has been removed, reconstruction focuses on restoring both appearance and function. Given SCCs often occur on sun-exposed and high-movement areas, careful planning is required in terms of the type of reconstructive procedure used.
Reconstruction options include:
Pathology results typically arrive within several days.
Patients with a history of SCC require closer observation than typical BCC patients because SCC has a higher chance of recurrence or spread.
Recovery is similar to other skin cancer removal procedures. You will be provided with a post-operative instruction booklet which outlines exactly how to look after the surgical site. Stitches will usually be removed the week following surgery. Sun protection, wound care, and avoidance of strenuous activity are recommended during healing.
Scar management includes sun avoidance, silicone therapy and regular massage.
Patients treated for SCC should attend regular skin checks, often every 3–6 months for the first two years, then annually. This schedule is more frequent than for BCC because SCC carries a greater risk of recurrence and metastasis.
All surgeries carry risks, and SCC excision is no exception. Possible complications include: