In 2021, I began a spreadsheet of every patient I operated on who had a close or involved margin. Here are the details that I record:
I review this list each month to extract lessons so I can get less positive margins in the future. They are the bane of my existence! Here are three things that I remind myself about before every operating list:
1. Watch out for fibrosing BCCs
A common pattern that developed early was how often fibrosing BCCs would be on my positive margin list. I now always take a bigger margin on these lesions. I also have a much lower threshold for referring these patients for Mohs surgery. This allows me to avoid the risk altogether.
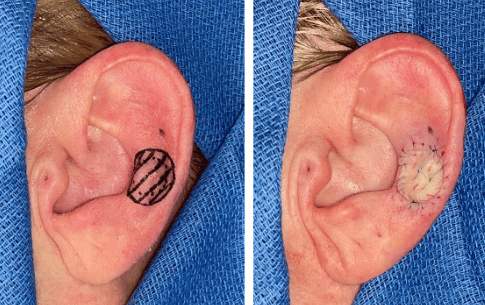
2. Make ear grafts bigger
My most common reconstruction on the ear is a full thickness skin graft. Full thickness skin grafts look great on the ear. Also, many patients say they don’t care what their ear will look like after surgery anyway. Due to these two factors, I often add 1-2mm to the margins when using a full thickness skin graft for the reconstruction. The end result is not noticeably different and I greatly reduce the risk of a positive margin.
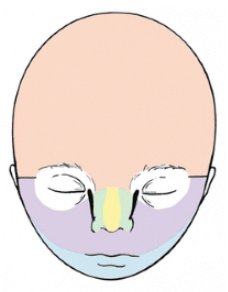
3. Be aggressive around embryonic fusion planes
During embryonic development, five facial processes fuse together to form the face. Research suggests that BCCs are more common along these fusion planes. Recurrences are also more common. I have a very high positive margin rate when I excise a lesion from one of these areas. This is especially true at the junction of the nose and cheek/upper lip (between purple and green in the photo below). I am now more aggressive with lesions in these areas. This often makes the reconstruction harder as it involves at least two cosmetic subunits.
I calculate my positive margin rate every month, and this usually sits between 3-5%. It’s tempting to try to push this number lower. But, I would have to take bigger margins for every patient I operate on. That would harm the 95-97% of patients who were going to get a clear margin anyway.
Until next time,
NS
